Table of Contents
I’ve grown cannabis long enough to know two things can be true at the same time: the plant can be genuinely useful in specific, well-defined medical contexts, and it can also be misused, misunderstood, or oversold—especially when the conversation turns to children and neurodevelopment.
Over the last few years, I’ve been asked the same set of autism caregiver questions in different forms: “Is there a cannabis option that helps with sleep?” “What about anxiety and meltdowns?” “How do I know what’s in the bottle?” “Is CBD safer than THC?” Those questions matter, but they live at the intersection of science, regulation, and real-world product quality—three areas that don’t always line up cleanly.
This article is a fresh, practical look at medical cannabis for autism from my side of the fence: the cultivation and quality-control side.
In this piece I’ll use cannabis, marijuana, and weed as everyday synonyms, because that’s how most people search and talk about the plant. I’m focused on product quality and cultivation fundamentals, not on promises.
I’m not a clinician, and I’m not offering medical advice. I am a hands-on cultivator who has selected genetics, dialed in environments, and chased cannabinoid profile consistency across multiple harvests. I’ve also watched how quickly a promising idea can become risky when dosing is improvised, labeling is sloppy, or products are stored like candy in a kitchen drawer.
If you’re researching medical cannabis for autism, I want you to walk away with three things:
- A realistic snapshot of what the research does and doesn’t show today
- A safety-first framework for evaluating products and handling them around kids
- A grower’s view of why “consistent” matters—how CBD-dominant genetics, careful environment control, and third-party lab testing change the conversation
What the research says (and what it still can’t say)

When I read the medical literature, I try to separate three categories:
- Core autism traits (social communication differences and repetitive behaviors)
- Common co-occurring challenges (sleep problems, anxiety, irritability, aggression, sensory overwhelm)
- Side effects and safety signals (sedation, appetite changes, GI upset, interactions, accidental ingestion)
The most responsible summary I can give is this: evidence is still limited, effects vary by individual, and the best signals so far are often in co-occurring symptoms rather than “core” autism traits.
A 2025 updated systematic review (covering seven studies and 494 patients) reported preliminary, modest benefits in areas like sleep, anxiety, social interaction, and some behavioral outcomes, while also noting inconsistent responses and the need for larger controlled trials.
Other reviews have reached similar conclusions: there’s interest and a plausible biological pathway, but the overall quality and size of studies remain a constraint, and results are mixed across endpoints.
That’s the first reason families end up with autism caregiver questions that sound like product-shopping questions. The science hasn’t converged on a simple protocol, so the burden shifts to product quality, dosing oversight, and risk management.
Why the endocannabinoid system keeps showing up in autism research
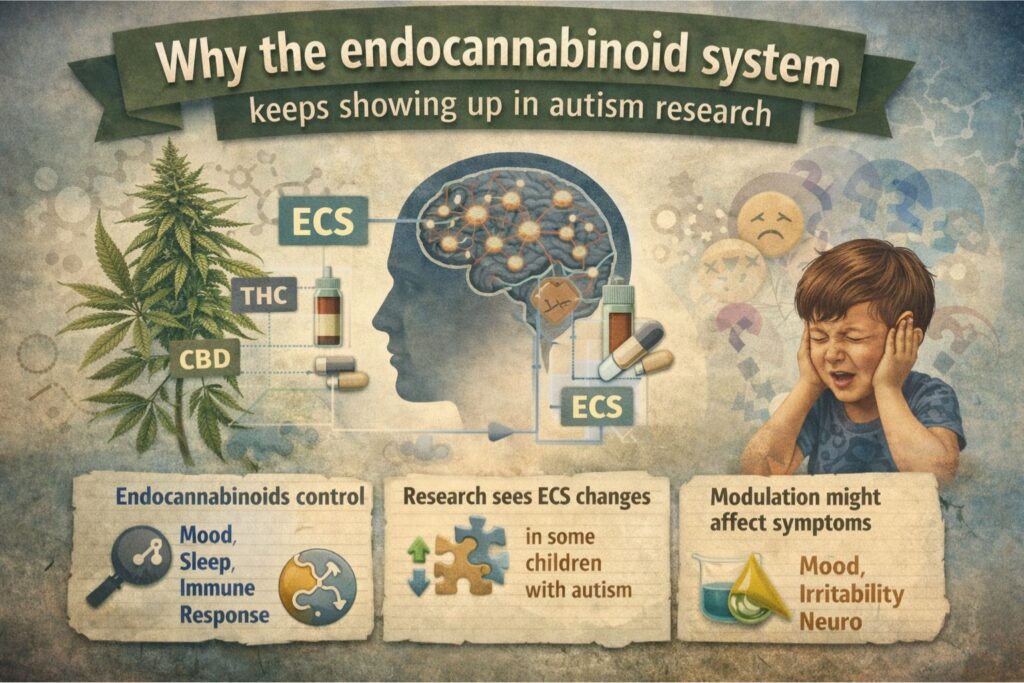
One reason cannabis gets discussed in autism circles is the endocannabinoid system (ECS). The ECS is a signaling network involved in neuromodulation, stress response, appetite, and immune signaling, among other functions. Researchers have explored whether ECS differences show up in autism and whether modulating ECS pathways might affect certain symptoms.
Human studies have reported signals such as lower circulating levels of certain endocannabinoids in some children with autism, though this is still an evolving area.
As a grower, the ECS angle matters because it explains why different cannabinoid ratios can produce very different effects in different people. It also explains why one child’s “calming” can be another child’s “over-sedation,” and why a product with the same label but different chemistry can behave like a completely different drug.
That’s where cannabinoid profile consistency becomes more than a marketing phrase—it becomes a safety issue.
CBD, THC, and ratios: the nuance that gets lost online
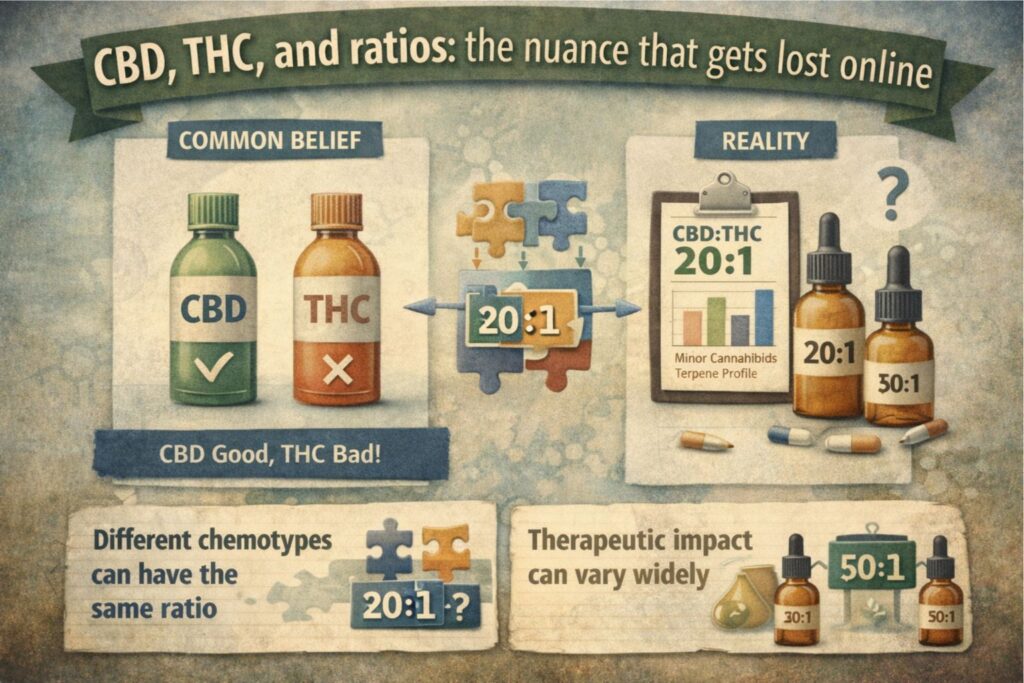
Most public conversations about cannabis and kids get simplified into “CBD good, THC bad.” Real life isn’t that clean.
- CBD (cannabidiol) is non-intoxicating and has been studied in multiple pediatric contexts.
- THC (tetrahydrocannabinol) is intoxicating, can impair coordination and judgment, and carries higher risk for adverse effects—especially when dosage is uncertain or products are accidentally ingested.
In the autism context, many clinical and observational reports focus on CBD-rich formulations, sometimes with small amounts of THC.
If you’re researching medical cannabis for autism, treat “ratio” as a shorthand, not a guarantee. Even the same stated ratio can feel different if the product’s minor cannabinoids and terpene profile change, or if the extract was made from a different chemotype.
From a cultivator’s standpoint, CBD-dominant genetics doesn’t automatically mean “predictable results,” but it does move the odds toward a more stable starting point. I’ve run CBD-dominant genetics that stayed within a tight window across harvests, and I’ve also seen CBD lines that swing more than expected between phenotypes.
That phenotype variation is exactly why third-party lab testing should be non-negotiable for anything described as “medical.”
Safety realities: children, edibles, and accidental ingestion
If there’s one part of this conversation I won’t soften, it’s child safety.
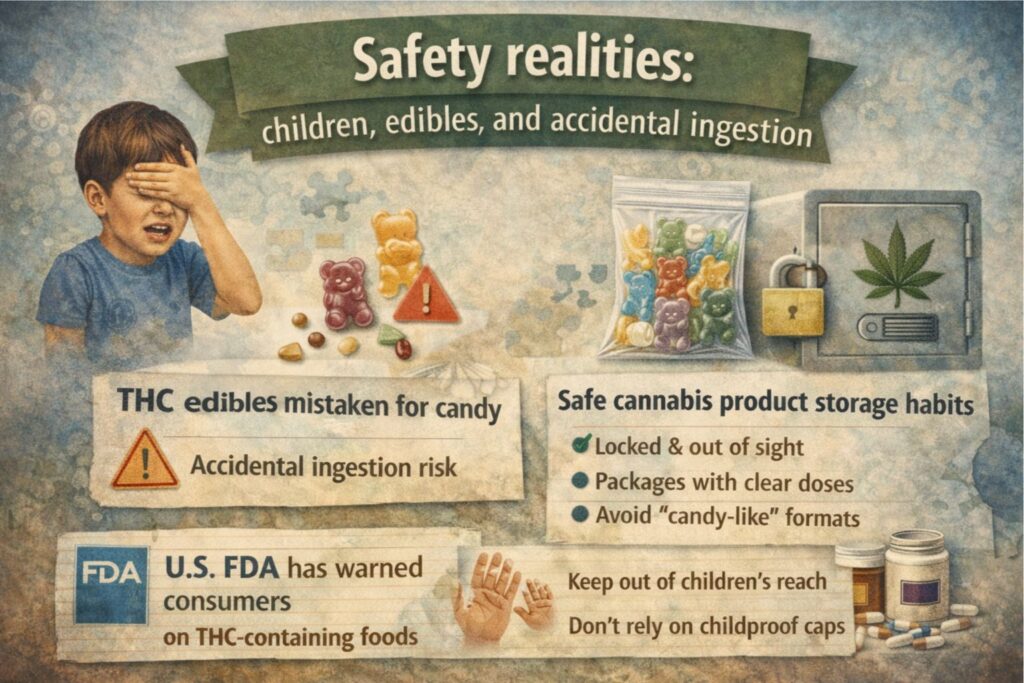
Accidental ingestion is a documented risk with THC-containing products, especially marijuana edibles that resemble common snacks. I’ve seen weed gummies stored like regular treats, and that’s exactly how mistakes happen.
Even if you live somewhere cannabis is legal, or you have a physician-supervised plan, safe storage cannabis products practices are essential. I treat cannabis the way I treat concentrated nutrients and pesticides in the grow room: always secured, clearly labeled, and never stored where “curious hands” can reach.
Here are my baseline safe storage cannabis products rules:
- Store all products locked, out of sight, and separate from regular food
- Keep products in original packaging with clear dosage information
- Avoid “candy-like” formats in households with children whenever possible
- Assume visitors may not understand what a product is—plan for that
If you only remember one thing from this article about medical cannabis for autism, remember this: safety isn’t a footnote. It’s the foundation.
What I look for in products when people ask me autism caregiver questions
Because I’m on the cultivation side, I can’t recommend a product for a specific person. But I can tell you how I evaluate product credibility when autism caregiver questions come up.
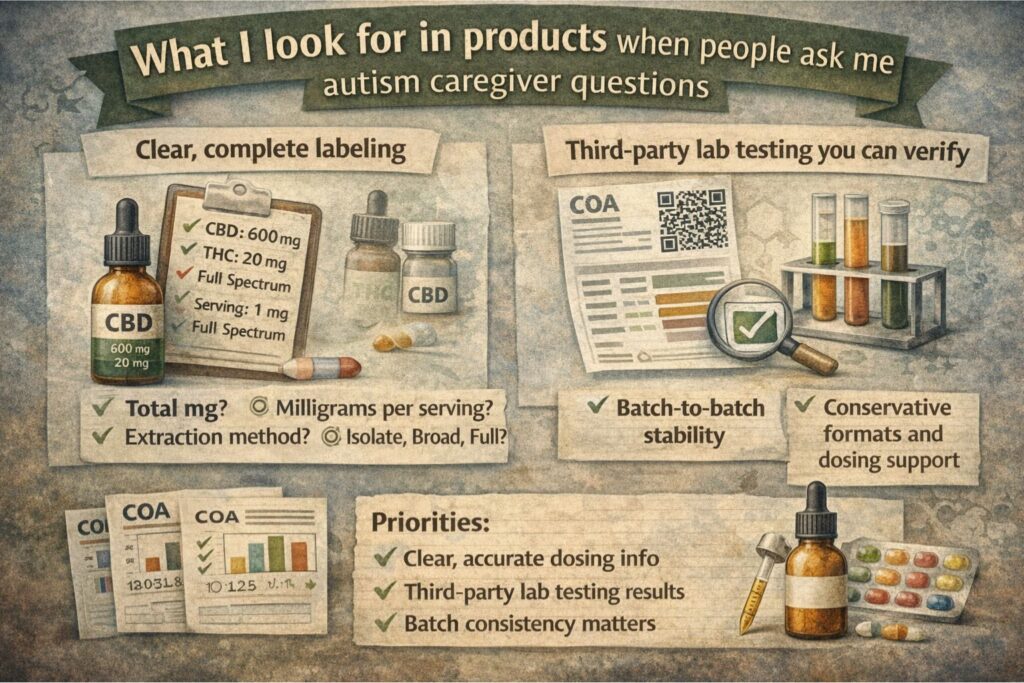
1) Clear, complete labeling
A credible product label should make it easy to answer:
- How many milligrams of CBD and THC are in a full container?
- How many milligrams are in one serving?
- What is the extraction method?
- Is it broad-spectrum, isolate, or full-spectrum cannabis extract?
If the label can’t answer those questions, I don’t trust it.
2) Third-party lab testing you can verify
Third-party lab testing should be accessible via a QR code or batch number. I want to see:
- Cannabinoid potency (CBD, THC, and ideally a few minors)
- A terpene panel, if relevant to the product type
- Contaminant screening (microbials, heavy metals, pesticides, residual solvents)
Third-party lab testing is the best reality check we have in a market where products can vary significantly between batches. Third-party lab testing also protects consumers from label drift, where the stated numbers aren’t close to the actual numbers.
3) Batch-to-batch stability
If a product is being used in a medical context, batch consistency matters. Ask whether the manufacturer can show multiple certificates over time. In my world, cannabinoid profile consistency is a tracked metric, not a vibe.
4) Conservative formats and dosing support
If a clinician is involved, the clinician should guide dosing. From a risk perspective, liquid formats allow smaller, more adjustable increments than “one gummy = one dose.” Many families searching medical cannabis for autism are really searching for controlled, measurable dosing.
That’s also where the topic of microdosing THC sometimes enters the conversation. Microdosing THC is not something I’d ever suggest casually, especially in pediatric situations. If it is discussed, it should be clinician-led, data-driven, and tightly controlled.
A grower’s view: why consistency starts with genetics
When people imagine “medical cannabis,” they often picture a dispensary shelf. I picture the opposite: a controlled environment, careful recordkeeping, and a process designed to reduce variation.
In practice, cannabinoid profile consistency begins with CBD-dominant genetics that have been selected for stability.
Even then, you still need to manage:
- Phenotype variation (different expressions from the same seed line)
- Environmental swings (temperature, humidity, light intensity)
- Nutrition and stress (which can shift secondary metabolite expression)
- Harvest timing (which can change cannabinoid and terpene balance)
If you’re a home grower, the best way to reduce variation is to select a keeper phenotype, then maintain a stable environment and repeatable harvest and post-harvest steps. If you’re shopping seeds, it’s worth asking the seed bank how the line was worked and whether it was selected for stable cannabinoid expression.
Seed-shopping terms I see most (and how I translate them)
When someone is browsing a seed bank, the search terms usually sound like this:
- feminized seeds that won’t produce males
- autoflowering seeds for small tents or quick cycles
- indica, sativa, or hybrid descriptors (useful for a rough idea, but not a guarantee)
- CBD-forward options, or low-THC selections
- discreet shipping and delivery timelines to a specific region
Here’s how I translate those terms as a cultivator.
Feminized seeds help reduce the odds of accidental pollination, which matters if you’re trying to keep cannabinoid profile consistency. Autoflowering seeds can be great for beginners, but they make it harder to run an identical plant again and again, which is why I lean photoperiod for repeatability.
If you’re new to germination, keep it boring: clean water, stable warmth, and a gentle medium. Most failed starts come from drowning seeds, letting them dry out, or swinging temperatures. Once seedlings are up, the next common problem I see is nutrient burn or nutrient deficiency from chasing an aggressive feeding schedule. Slow, measured adjustments beat guesswork—especially if your end goal is a stable CBD-rich harvest.
This is also where people ask can I buy cannabis seeds online. The better question is whether ordering marijuana or weed seeds is permitted where you live, and whether you can follow local rules safely. I can’t give legal advice, but I can say this: verify your local regulations before you order anything, and don’t rely on outdated forum posts.
Environment targets I use to reduce variation
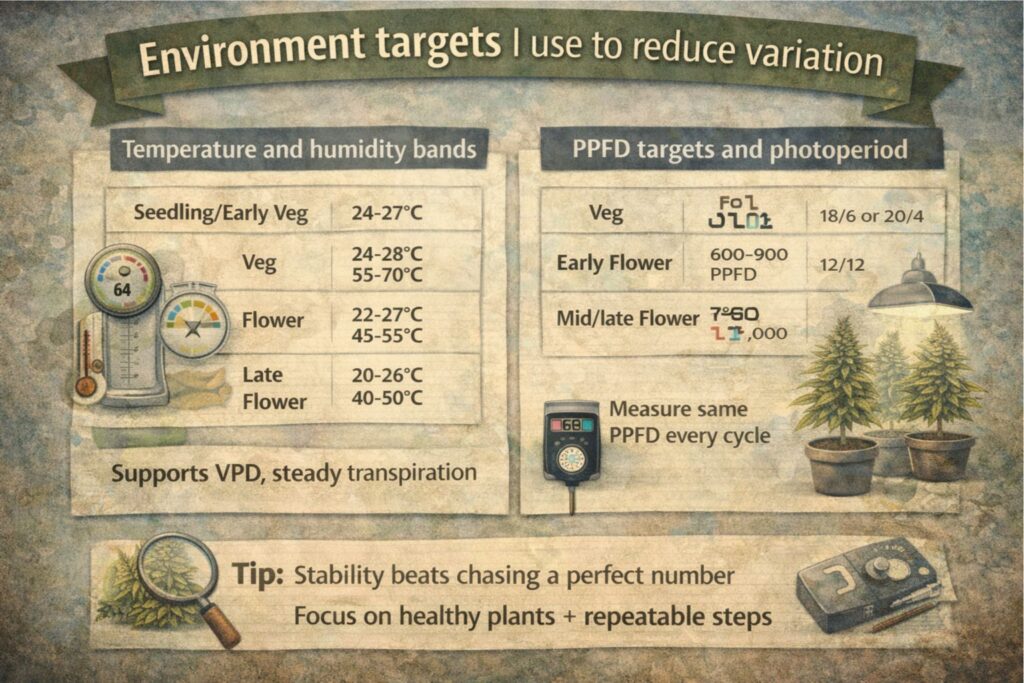
Below are ranges I’ve used successfully in indoor grows. They’re not commandments, but they’re realistic bands that help reduce surprises.
Temperature and humidity bands
- Seedling/early veg: 24–27°C with 65–75% RH
- Veg: 24–28°C with 55–70% RH
- Flower: 22–27°C with 45–55% RH
- Late flower: 20–26°C with 40–50% RH (to reduce mold risk)
These ranges support VPD for indoor cannabis management. When growers talk about VPD for indoor cannabis, what they usually mean is keeping transpiration steady so the plant can feed predictably.
A simple way to use VPD for indoor cannabis is to avoid big day-to-night swings and avoid wet leaf conditions late in flower. I keep airflow high, dehumidification steady, and I don’t let perfect numbers become an excuse to ignore plant signals.
PPFD targets and photoperiod
For photoperiod plants:
- Veg: 300–600 PPFD (18/6 or 20/4 light cycle)
- Early flower: 600–900 PPFD (12/12)
- Mid/late flower: 700–1,000 PPFD if the canopy and nutrition can support it
When I’m growing with a medical outcome in mind, I still use performance lighting targets, but I track PPFD for medical grows in a way that emphasizes repeatability over maximum. PPFD for medical grows is less about chasing the highest number and more about hitting the same number, the same way, every cycle.
If you’re new, don’t guess. Measure. PPFD for medical grows is one of the easiest variables to stabilize with a decent meter and consistent hanging heights.
Nutrition: EC/PPM guardrails
I run different nutrient strategies in soil and hydro, but the idea is the same: avoid extremes that create stress.
- Seedling: gentle feed, often under 0.6–0.8 EC depending on water and medium
- Veg: commonly 1.0–1.6 EC depending on cultivar and growth rate
- Flower: commonly 1.4–2.0 EC, with careful monitoring for burn
Nutrient burn doesn’t just reduce yield; it can change how a plant expresses. If you’re chasing cannabinoid profile consistency, you want healthy, steady growth rather than dramatic push and pull cycles.
Soil vs hydro for consistent chemistry
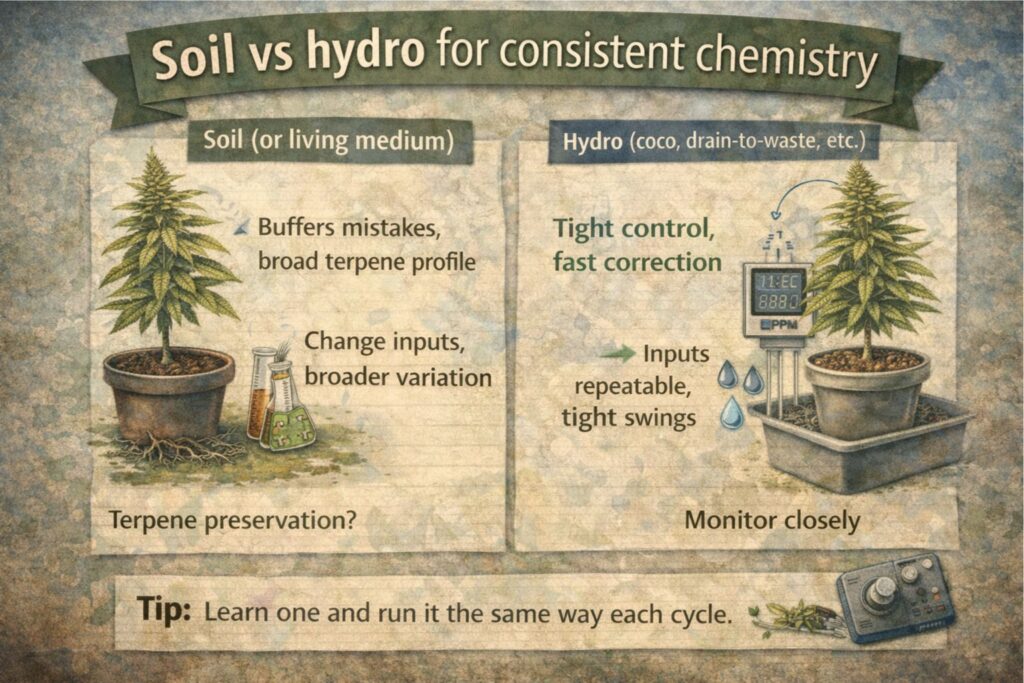
This is one of the most common cultivation queries I hear.
Soil (or a soil-like living medium) can buffer mistakes and often produces a broad terpene expression—useful for terpene preservation goals—but it can also introduce more variability if your inputs change.
Hydro (including coco) gives you tighter control and faster correction. If your aim is cannabinoid profile consistency, hydro can make it easier to repeat the same nutrition and irrigation patterns. The trade-off is that mistakes happen fast, and you need to monitor more often.
Either system can work. What matters is that you pick one approach and run it the same way long enough to learn it.
Training and canopy management: my practical approach
I’m not chasing extreme plant training for medical grows. I’m chasing uniformity.
What I use most often:
- Topping in early veg to create an even canopy
- Low-stress training to spread branches and reduce shading
- Selective defoliation in flower to improve airflow and reduce humidity pockets
Aggressive training can increase stress. Stress can increase variability. When people are researching medical cannabis for autism, they often don’t realize that grow stress can translate into chemistry swings from harvest to harvest.
Harvest timing and why it matters

Harvest timing can shift the final cannabinoid balance. In practice, I watch:
- Trichome development (and not just color—also density and distribution)
- Aroma changes (a proxy for terpene maturity)
- Plant posture and senescence (the plant tells you when it’s finishing)
This is another reason I avoid recommending strain names for specific needs. Even within the same line, harvest timing can change the experience. If you want terpene preservation and stable cannabinoid expression, harvest too early or too late and you may miss the profile you were aiming for.
Drying and curing: terpene preservation in real life
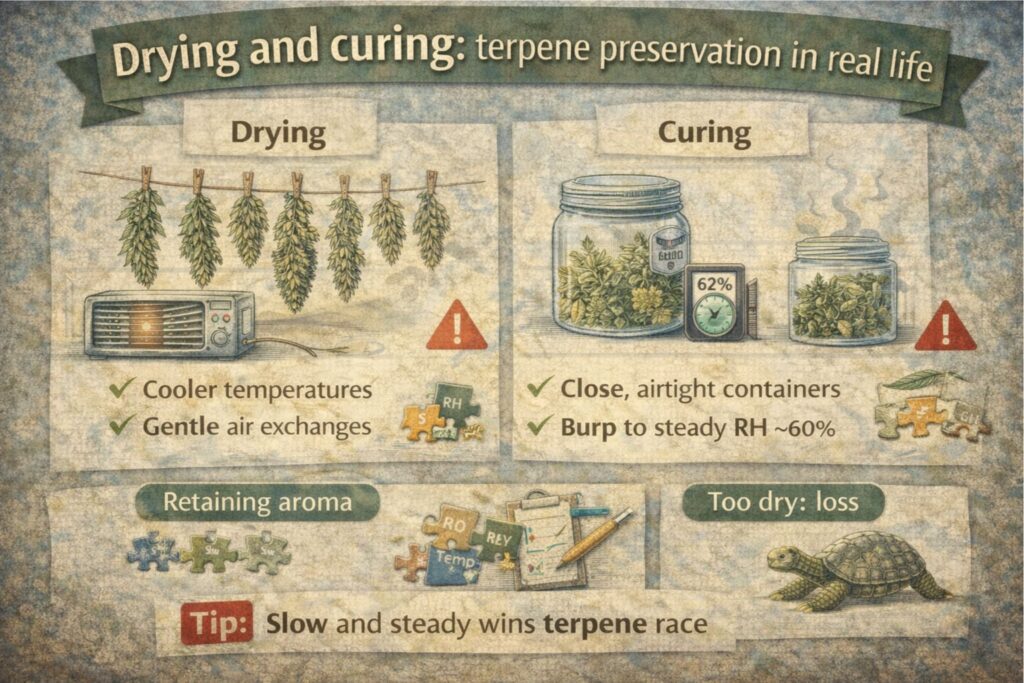
I’ll say it plainly: terpene preservation is where most home growers lose the best version of their crop.
My usual targets:
- Dry at about 18–20°C and 55–60% RH
- Keep airflow gentle, not blasting
- Aim for a slow dry that typically takes 10–14 days (sometimes longer depending on density)
After drying, I cure in sealed containers, burping as needed, until moisture is stable. This is terpene preservation, but it’s also safety: overdry becomes harsh, underdry risks mold.
Terpene preservation is also tied to storage. Heat, oxygen, and light degrade aroma compounds. If you care about terpene preservation, treat your jars like you treat any sensitive botanical product: cool, dark, and sealed.
Extraction and formulations: why full-spectrum isn’t automatically better
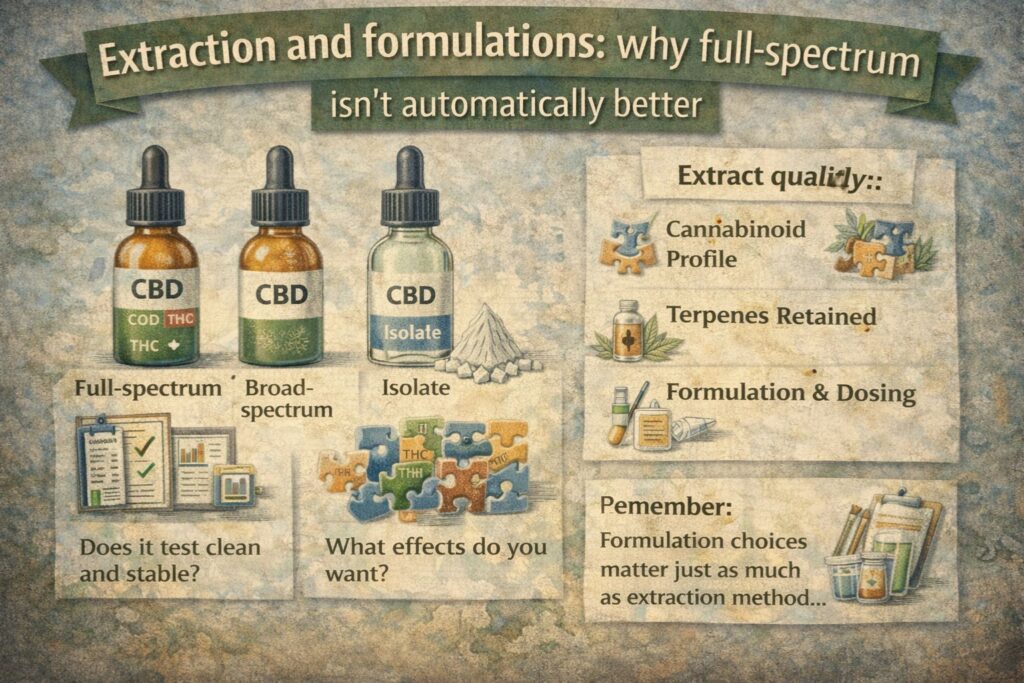
Many consumers prefer a full-spectrum cannabis extract because it contains more than just CBD or THC. That preference makes sense, but it also increases complexity.
A full-spectrum cannabis extract can vary more from batch to batch unless the manufacturer standardizes it. A full-spectrum cannabis extract also concentrates whatever contaminants were present in the source material if the grow and processing aren’t clean.
So my rule is simple: if you’re considering a full-spectrum cannabis extract, you should be even more strict about third-party lab testing and batch documentation.
Microdosing and supervision: where I draw a hard line

Online discussions often push microdosing THC as a universal solution. Microdosing THC is not universal, and it is not low-risk by default.
Microdosing THC is a dosing strategy that assumes:
- A known and reliable concentration
- A measured administration method
- A plan for monitoring effects and side effects
- A clinician who can adjust the plan, especially with children
When the subject is medical cannabis for autism, microdosing THC should never be treated like a DIY experiment. If you take anything from this section, let it be that microdosing THC belongs in a supervised context, not in a comment thread.
Seed selection for growers: photoperiod vs autoflowering, and why I choose differently
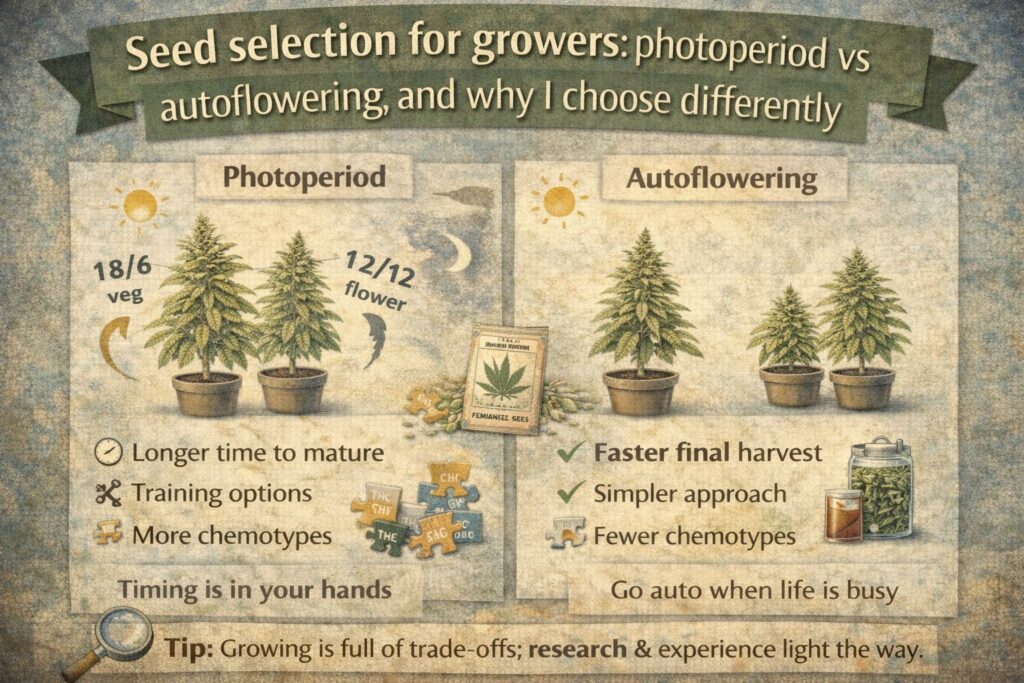
People often ask me which type is better. For consistency, I usually prefer photoperiod plants because I can keep a mother and run clones. Clones reduce phenotype variation and improve cannabinoid profile consistency over time.
Autoflowering plants are convenient and fast, and they can be great for beginners. But they’re harder to clone and keep identical, which can make consistency harder.
If you’re growing for personal use, choose based on your setup and goals:
- Need speed and simplicity? Autoflowering can fit.
- Need repeatable chemistry? Photoperiod with a selected keeper is often the best path.
This is also where CBD-dominant genetics and careful selection matter. CBD-dominant genetics in feminized seed form can work well, but nothing beats the repeatability of a proven keeper cut when your aim is cannabinoid profile consistency.
A practical checklist for people researching medical cannabis for autism
Below is the checklist I share when autism caregiver questions come up. It’s not medical advice; it’s a quality and safety checklist.
Product and safety checklist
- Confirm third-party lab testing exists for the exact batch you have
- Confirm the label lists total milligrams and milligrams per serving
- Avoid products packaged like candy or snacks
- Use safe storage cannabis products habits: locked, separate, labeled
- Keep a written log if a clinician recommends a trial (timing, dose, effects, side effects)
- Watch for sedation, GI upset, appetite changes, or mood changes and report them to a clinician
If you’re a home grower checklist
- Start with CBD-dominant genetics selected for stability
- Control VPD for indoor cannabis to reduce stress-driven swings
- Measure PPFD for medical grows and keep it stable across cycles
- Avoid nutrition extremes; track EC and runoff
- Harvest based on plant maturity signals, not calendar days
- Prioritize terpene preservation through slow drying and cool storage
FAQ: long-tail questions I hear most often
Is medical cannabis for autism proven to work?
No. Evidence is still limited, and responses vary. Current reviews describe preliminary, modest benefits in some co-occurring symptoms (like anxiety and sleep) for some individuals, but they also emphasize inconsistent outcomes and the need for larger controlled trials.
Does CBD help autism symptoms?
Some studies and reviews have explored CBD-rich products in autism, with mixed results and a focus on co-occurring symptoms rather than definitive changes in core traits. The strongest takeaway is that research is ongoing and not conclusive.
Is THC safe for children?
Accidental ingestion of THC products is a recognized risk, especially with edible formats that resemble snacks.
If THC is ever part of a medical plan, it should be clinician-supervised, carefully dosed, and stored securely using safe storage cannabis products practices.
What does full-spectrum mean, and is it better?
A full-spectrum cannabis extract generally includes multiple cannabinoids and other plant compounds. Some people prefer it, but it requires strong batch control and third-party lab testing because composition can vary and contaminants can concentrate.
How can a grower improve consistency for CBD-rich harvests?
I focus on cannabinoid profile consistency by combining CBD-dominant genetics with stable environment control. In practice that means managing VPD for indoor cannabis, measuring PPFD for medical grows, and keeping nutrition and irrigation patterns repeatable. I also prioritize terpene preservation in drying and storage because post-harvest swings can change the experience as much as the grow.
Should I try microdosing THC?
Microdosing THC is a dosing strategy that still carries risk if concentration or administration is uncertain. In the context of medical cannabis for autism, microdosing THC should be discussed only with a qualified clinician who can monitor outcomes, side effects, and interactions.
Can I make my own tincture at home?
Home extraction introduces risks: inaccurate potency, contamination, and unsafe storage around children. If you’re in a household asking autism caregiver questions, I strongly prefer clinically guided products with third-party lab testing and child-safe storage.
Are there legal considerations?
Cannabis laws vary widely by country, state, and region, and they change over time. Treat any legal information you read online as something to verify locally. If you choose to purchase seeds or cannabis products, do so only where permitted and follow local requirements.
Final thoughts from the grow room
I understand why medical cannabis for autism is such a persistent search topic. Families are looking for options, and the existing medication landscape doesn’t always meet every need. But natural doesn’t automatically mean safe, and CBD-rich doesn’t automatically mean consistent.
From my perspective, the most helpful contribution I can make is to pull the focus back to fundamentals: product credibility, third-party lab testing, safe storage cannabis products habits, and (for growers) the unglamorous work of environmental control, PPFD for medical grows tracking, VPD for indoor cannabis management, and terpene preservation after harvest.
If you’re here because you have autism caregiver questions, I hope this gave you a clear map of the trade-offs—and a safer way to evaluate the information you’ll see online, whether you call it cannabis, marijuana, or weed.